AORTIC ROOT ANEURYSMS
Click on anatomy picture to enlarge
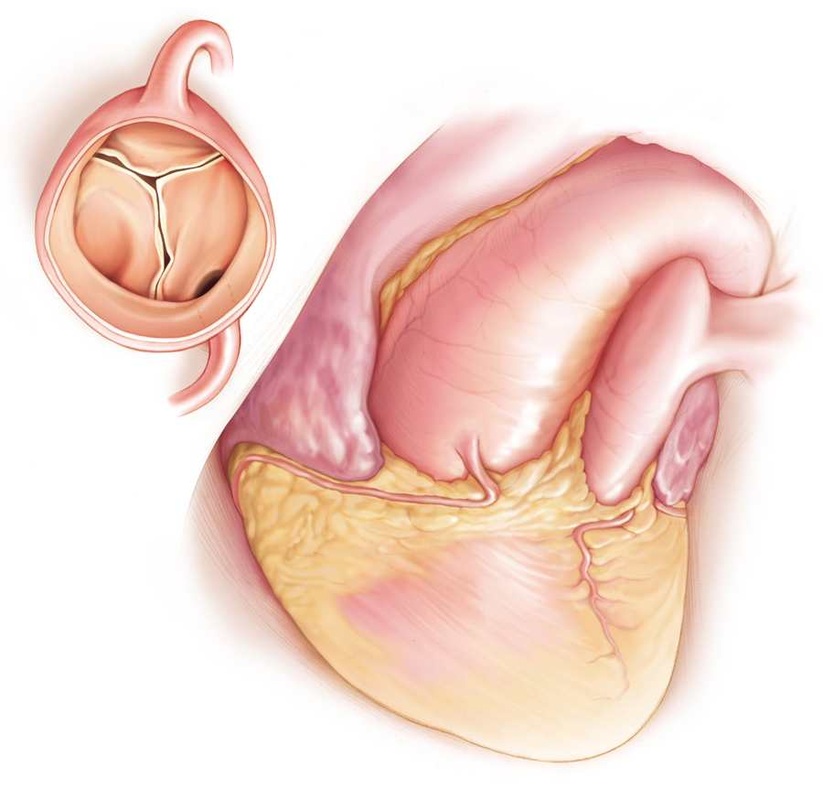
As the word implies, the aortic root is the first portion of the thoracic aorta that joins the outflow from the left ventricle (main heart pump) and to the remaining segments of the aorta. The aortic root is the first two to three centimeters of the aorta comprising of the aortic valve, annulus, aortic sinuses, and opening to the coronary arteries. This small portion of the aorta has numerous structures, all in close proximity to one another. Please refer to the anatomy section and other figures in this section to enhance your visual understanding of this area of the thoracic aorta.
Aortic root aneurysms are not very common aortic aneurysms. The typical causes or conditions associated with aortic root aneurysms are:
· annulo-ectasia,
· Marfan syndrome,
· Bicuspid aortic valve,
· Loey-Dietz Syndrome
· Inflammatory/autoimmune diseases
In general, most aortic root aneurysms are associated with dilation of the tubular portion of the ascending aorta. The aortic root aneurysms associated with Marfan syndrome have the typical “pear-like” appearance with quite normal aortic diameter measurements up until the aortic arch (see 3-D CT scan above).
Aortic root aneurysms are not very common aortic aneurysms. The typical causes or conditions associated with aortic root aneurysms are:
· annulo-ectasia,
· Marfan syndrome,
· Bicuspid aortic valve,
· Loey-Dietz Syndrome
· Inflammatory/autoimmune diseases
In general, most aortic root aneurysms are associated with dilation of the tubular portion of the ascending aorta. The aortic root aneurysms associated with Marfan syndrome have the typical “pear-like” appearance with quite normal aortic diameter measurements up until the aortic arch (see 3-D CT scan above).
Symptoms
Aortic root aneurysms do not usually cause an individual to have any specific symptom. Like other thoracic aortic aneurysms, root aneurysms are commonly found in asymptomatic (no symptoms) patients when undergoing a radiologic or cardiac study like a CT scan or echocardiogram. In some cases the aortic root aneurysm will lead to certain symptoms such as dull chest pain, angina (chest pain on exercise) or shortness of breath. As mentioned, the aortic root involves structures such as the aortic valve, coronary arteries, and aortic annulus. As an aortic root aneurysm expands, the fine balance between these three structures is distorted. The expansion leads to outwards pull on the aortic valve leading to the inability of the aortic valve to close properly. The valve leaflets (like doors) no longer meet in the center and maintain a tight seal, which normally prevents blood to reenter the heart. Normally, blood is ejected or pumped out of the left ventricle through the aortic valve into the ascending aorta. When the aortic valve seal no longer functions the blood returns into the left ventricle (pump). The leakage of blood back into the left ventricle can be tolerated for quite a long time however, in time, the patient will begin to experience shortness of breath, fatigue and chest pain. In addition, as the leakage (aortic valve regurgitation) increases the amount of blood that passes through the opening of the coronary arteries decreases. An individual can develop chest pain “angina” when exercising---as the heart demands more blood to meet the needs of the body. The symptoms, although not only associated with aortic root aneurysms, can be the first symptoms that one may have an aneurysm in this portion of the aorta.
Aortic root aneurysms are associated with acute aortic dissections. Therefore, elective repair can prevent this catastrophic event especially in patients with Marfan syndrome, Loey-Dietz syndrome and other genetically related aneurysm. Unfortunately, the first time a patient may become aware of this underlying aortic aneurysm and/or connective tissue disorder is at the time of the acute aortic dissection. This may be the case of young patients who were not corrected diagnosed for Marfan Syndrome because they do not manifest the typical characteristics.
In general, elective repair is considered when the risk of rupture is greater than the risk of surgery. The general consensus is to operate when the aortic root has reached 5.5 cm in good surgical candidates. The degree of aortic valve leakage (aortic valve regurgitation), symptoms, the size of the left ventricle (the result of overload on the left ventricle from the aortic leakage) all need to be considered when making the decision to proceed with elective repair. The rate of growth of the aortic root must also be considered. When an aortic root aneurysm expands by more than 0.5 cm in one year, one may consider to elective repair regardless if the diameter is less than 5.5 cm. In other situations, the degree of aortic valve regurgitation and the size of the left ventricle may influence earlier surgical intervention.
Sign up for Formal Aortic Aneurysm Surveillance Program, one of the largest programs in the US-more than 1400 patients.
Aortic root aneurysms are associated with acute aortic dissections. Therefore, elective repair can prevent this catastrophic event especially in patients with Marfan syndrome, Loey-Dietz syndrome and other genetically related aneurysm. Unfortunately, the first time a patient may become aware of this underlying aortic aneurysm and/or connective tissue disorder is at the time of the acute aortic dissection. This may be the case of young patients who were not corrected diagnosed for Marfan Syndrome because they do not manifest the typical characteristics.
In general, elective repair is considered when the risk of rupture is greater than the risk of surgery. The general consensus is to operate when the aortic root has reached 5.5 cm in good surgical candidates. The degree of aortic valve leakage (aortic valve regurgitation), symptoms, the size of the left ventricle (the result of overload on the left ventricle from the aortic leakage) all need to be considered when making the decision to proceed with elective repair. The rate of growth of the aortic root must also be considered. When an aortic root aneurysm expands by more than 0.5 cm in one year, one may consider to elective repair regardless if the diameter is less than 5.5 cm. In other situations, the degree of aortic valve regurgitation and the size of the left ventricle may influence earlier surgical intervention.
Sign up for Formal Aortic Aneurysm Surveillance Program, one of the largest programs in the US-more than 1400 patients.
Surgical Considerations
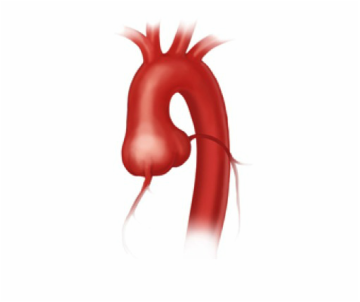
Typical aortic root aneurysm of patient with Marfan syndrome
Patients with connective tissue disorders such as Marfan and Loey-Dietz Syndromes are offered elective aortic root replacement at smaller aortic diameters. Patents with Loey-Dietz syndrome have a very aggressive aortic condition resulting in acute aortic dissections at very small aortic diameters. In theses patients, surgical repair is recommended at aortic diameter of 4.5 cm. In Marfan syndrome, the recommended aortic diameter is 5.0 cm, although, if there is a strong family history of aortic dissection, earlier repair should be offered. In patients with Turner’s Syndrome, it seems reasonable to offer surgical repair at a aortic diameter of 4.5 cm or aortic index of >2.5 cm/mm2.
Types of Operations: Bentall Procedure
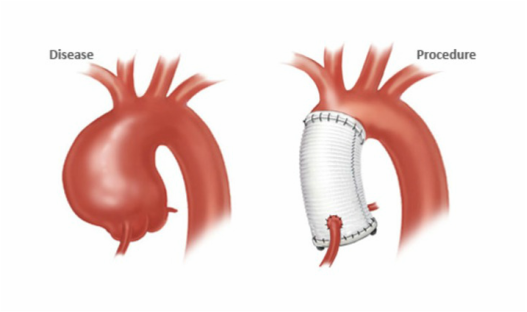
Bentall Procedure
The gold standard treatment for aortic root aneurysms is the Bentall procedure which involves replacing the ascending aorta and the aortic valve. The aortic valve can be replaced with either a bovine (cow) or porcine (pig) valve. The largest series of Bentall operations can be found through Pubmed. However, aortic valve-sparing root replacements are a very good option for patients with connective tissue disorder, young patients, patients who can not take anti-coagulants (blood thinners) and is a personal life-style choice. In these operations the aortic tissue surrounding the aortic valve is removed along with the ascending aorta. The aortic vale and it's support structures are sutured to a tube graft (see below). If patients are carefully selected for theses operations, the operation can be quite durable.
Valve-sparing root replacement
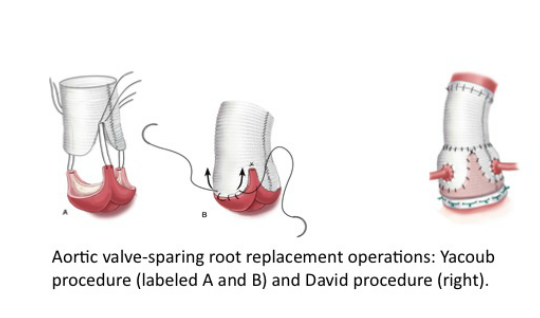
Valve-sparing aortic root replacement
As described above the aortic valve is re-implanted into the prosthetic tube graft and carefully sutured to re-establish a functioning aortic valve. Occasionally, the aortic valve needs additional repair at the time of the operation to achieve an adequate closure of the valve leaflets.
The long-term durability is dependent on many factors there proper consultation with centers that perform this operation frequently is important. The failure rate of valve-sparing aortic root operations is approximately 10% in 20 years. In such circumstances, the patient may be a candidate for re-repair or aortic valve replacement.
The long-term durability is dependent on many factors there proper consultation with centers that perform this operation frequently is important. The failure rate of valve-sparing aortic root operations is approximately 10% in 20 years. In such circumstances, the patient may be a candidate for re-repair or aortic valve replacement.
