Type B Aortic Dissection
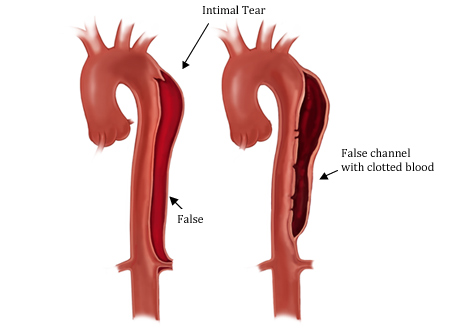
Illustration of Type B aortic dissection (acute and chronic)
A Type B aortic dissection occurs when there is an intimal tear present beyond the left subclavian artery. However, this tear can also form in the aortic arch. The false channel propagates distally into the descending and abdominal aorta. If the false channel travels toward the ascending aorta this is classified as a Type A aortic dissection. The passage of blood through the false channel can lead to complications such as spinal cord injury (paraplegia), lack of blood supply to the intestines (mesenteric ischemia) or lower extremities. The flow of blood in the false channel can cause these complications by pinching / narrowing off the flow of blood into the branches off the aorta.
Presentation
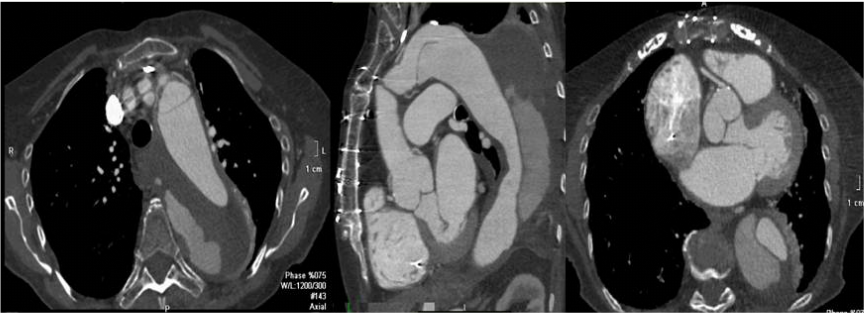
CTA showing Type B aortic dissection; the true lumen has the brighter contrast and the false channel has the gray tinted contrast.
Quick Facts:
- Overall, more than 60-80% of patients with type B aortic dissection have an elevated blood pressure at presentation.
- Another predominant feature in patients with aortic dissections is the history of cigarette smoking.
- Approximately 30-40% of patients have a history of atherosclerosis.
- Ten to twenty percent of patients have a history of a connective tissue disorders, prior cardiac or aortic surgery or aortic aneurysm.
- The most common presentation is severe, sharp, tearing, back pain. At times, the pain may feel like it is extending into your chest and abdomen.
- Approximately 90% of patients can be treated conservatively with blood pressure and heart rate control. The treatment is called “anti-impulse” therapy.
- Basically, the therapy consists of slowing down the heart rate and lowering the blood pressure with blood pressure medications designed to reduce the stress against the wall of the aorta. Surgery or endovascular therapies are performed when there are complications from the aortic dissection such as rupture or lack of blood to various organs (malperfusion). If there is rapid expansion in the size of the aorta in the first few days after the dissection, surgery or endovascular repair may be necessary.
- The diagnostic study of choice for Type B aortic dissection is a CT scan angiogram. A transesophageal echocardiogram (TEE), a specialized ultrasound, can be performed however its less efficient, more invasive, requires a cardiologist and sedation and may not be available at all hours.
Long-term outcomes with medical therapy
Patients require long-term follow-up to evaluate the rate of growth and size of the aorta. The first two years after an aortic disection is when the patient is at most risk of experiencing changes in the diameter of the descending thoracic aorta. The weakened thoracic aorta secondary to the aortic dissection can develop into an aneurysm. Therefore, patients will need to be seen and undergo either a MRA or CTA every 6 months during the first two years.
In studies dedicated to investigating the natural history of thoracic aortic aneurysms, patients with a chronic type B aortic dissection tended to have more aortic complications when the aortic diameter reached 5.5 to 6 cm.
Patients with a dissected aortic aneurysm of the descending thoracic aorta may need surgery or an endovascular stent repair when the diameter reaches 5.0-5.5 cm.
Sign up with our Formal Aortic Aneurysm Surveillance Program, one of the largest in the US-more than 1,400 patients.
In studies dedicated to investigating the natural history of thoracic aortic aneurysms, patients with a chronic type B aortic dissection tended to have more aortic complications when the aortic diameter reached 5.5 to 6 cm.
Patients with a dissected aortic aneurysm of the descending thoracic aorta may need surgery or an endovascular stent repair when the diameter reaches 5.0-5.5 cm.
Sign up with our Formal Aortic Aneurysm Surveillance Program, one of the largest in the US-more than 1,400 patients.
Endovascular Repair Of Acute Type B Aortic Dissection
In most cases medical management alone is sufficient to treat patients with a Type B aortic dissection. There are patients who develop a complication of the acute dissection such as rupture, malperfusion, or rapid aortic expansion may need an intervention. Its clear that in an acute event TEVAR (stent repair) has a role since it has less short-term morbidity and mortality over traditional open repair. In a recent trial TEVAR was better in managing patients with complications related to the aortic dissection and causing the false lumen to thrombose (clot off). In the longer term (>2 years), survival appeared to improve with TEVAR compared to medical management alone. The disadvantage of TEVAR compared to medical therapy alone was the patients treated with the stent had a higher number of strokes and spinal cord injuries related to the procedure. The placement of the TEVAR cause aortic remodeling,( one could interpret as healing of the aortic dissection) a term used to describe the appearance of the true lumen and false lumen. In general, one would like to see an increase in true lumen size and decrease in the false lumen size.
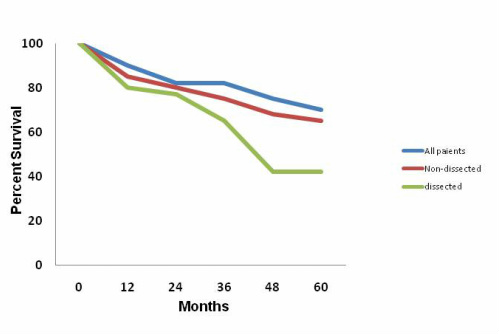
Long-term Survival of Patients with Chronic Type B Aortic
Dissection
In selective patients, surgery may become necessary for aortic complications or dramatic expansion in patients with chronic Type B aortic dissections. In a recent publication by our team, patients who survived one year after surgery had the same survival of a matched NY state population. The long-term death rate between the operated group and the matched group (gender and age) did not differ significantly. The need for further aortic interventions (other surgeries or stent) on the segment of aorta which was not replaced was very low.
Reference:
Zoli, S Etz CD, Mueller CS et al. Long-term Survival after open distal open repair of chronic aortic dissection. Ann Thorac Surg 2010 May;89(5):1258-66.
Reference:
Zoli, S Etz CD, Mueller CS et al. Long-term Survival after open distal open repair of chronic aortic dissection. Ann Thorac Surg 2010 May;89(5):1258-66.
Selected publications:
Zoli, S Etz CD, Mueller CS et al. Long-term Survival after open distal open repair of chronic aortic dissection. Ann Thorac Surg 2010 May;89(5):1258-66. (click on image)
|
Griepp RB, Ergin MA, Galla JD et al. Natural hisory of descending thoracic and thoracoabdominal aortic aneurysms. Ann Thorac Surg 1999 June ;67(6):1927-30. (click on image)
|
