Bicuspid Aortic Valve
What is a Bicuspid Aortic Valve?
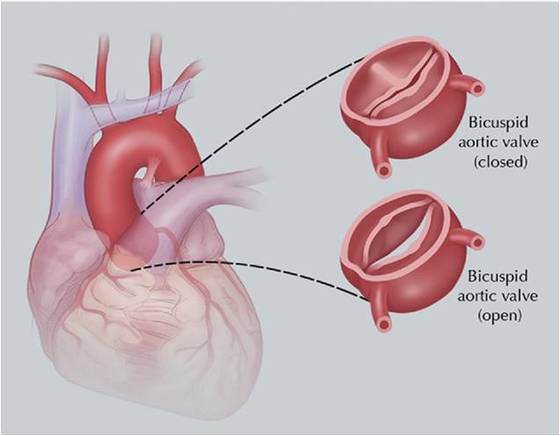
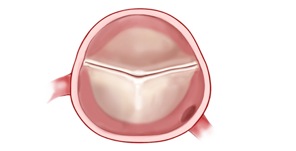
The aortic valve is the first valve the blood passes through after leaving the heart. In the open position, the valve manages the volume of blood that leaves the left ventricle (the main pump) and enters the ascending aorta. The aortic valve is commonly composed of three leaflets (doors) which close and does not allow blood to return back into the left ventricle. A bicuspid aortic valve only has two doors and appears like a “fish-mouth”.
How common is a bicuspid aortic valve?
In general, approximately 1-2% of the general population has a bicuspid aortic valve. The chance that another member of the family will have a bicuspid aortic valve increases to approximately 10%.
Does everyone with a bicuspid aortic valve need surgery?
No. Approximately one-third of patients will not need any intervention on their aortic valve. The common reasons for which an individual may need surgery are: infection (endocarditis), aortic stenosis (narrowing) and regurgitation (leakage).
Do bicuspid aortic valves last as long as trileaflet aortic valves?
No. In general, the bicuspid aortic valve will fail much earlier than trileaflet aortic valve. A patient with a diseased bicuspid aortic valve could expect to have surgery on the aortic valve in their 5th or 6th decade of life.
How do I know if I need surgery?
Most patient who need surgery will develop symptoms like chest pain, shortness of breath, fatigue, and syncope (loss of consciousness on exertion). You will need an annual echocardiogram by your cardiologist when the aortic valve begins to show signs of deterioration. The cardiologist will be looking with the echocardiogram for the degree of narrowing, leakage of the aortic valve, and how well the left ventricle is handling the changes with aortic valve. If the function of the left ventricle (ejection fraction) begins to decrease or the left ventricle begins to dilated or enlarge then he/she may refer you for surgery.
Why do I need to worry about my ascending aorta?
Patients with a bicuspid aortic valve are also at risk of developing an aneurysm of the ascending aorta. Depending on the criterion used to define an aneurysm, up to 60% of patients with a bicuspid aortic valve will have dilatation of the ascending aorta.
What causes an ascending aortic aneurysm in patients with a bicuspid aortic valve?
There is some preliminary data to suggest that the same genetic mutation that cause the formation of the bicuspid aorta has a role in the weakening of the aortic wall.
The aortic valve is the first valve the blood passes through after leaving the heart. In the open position, the valve manages the volume of blood that leaves the left ventricle (the main pump) and enters the ascending aorta. The aortic valve is commonly composed of three leaflets (doors) which close and does not allow blood to return back into the left ventricle. A bicuspid aortic valve only has two doors and appears like a “fish-mouth”.
How common is a bicuspid aortic valve?
In general, approximately 1-2% of the general population has a bicuspid aortic valve. The chance that another member of the family will have a bicuspid aortic valve increases to approximately 10%.
Does everyone with a bicuspid aortic valve need surgery?
No. Approximately one-third of patients will not need any intervention on their aortic valve. The common reasons for which an individual may need surgery are: infection (endocarditis), aortic stenosis (narrowing) and regurgitation (leakage).
Do bicuspid aortic valves last as long as trileaflet aortic valves?
No. In general, the bicuspid aortic valve will fail much earlier than trileaflet aortic valve. A patient with a diseased bicuspid aortic valve could expect to have surgery on the aortic valve in their 5th or 6th decade of life.
How do I know if I need surgery?
Most patient who need surgery will develop symptoms like chest pain, shortness of breath, fatigue, and syncope (loss of consciousness on exertion). You will need an annual echocardiogram by your cardiologist when the aortic valve begins to show signs of deterioration. The cardiologist will be looking with the echocardiogram for the degree of narrowing, leakage of the aortic valve, and how well the left ventricle is handling the changes with aortic valve. If the function of the left ventricle (ejection fraction) begins to decrease or the left ventricle begins to dilated or enlarge then he/she may refer you for surgery.
Why do I need to worry about my ascending aorta?
Patients with a bicuspid aortic valve are also at risk of developing an aneurysm of the ascending aorta. Depending on the criterion used to define an aneurysm, up to 60% of patients with a bicuspid aortic valve will have dilatation of the ascending aorta.
What causes an ascending aortic aneurysm in patients with a bicuspid aortic valve?
There is some preliminary data to suggest that the same genetic mutation that cause the formation of the bicuspid aorta has a role in the weakening of the aortic wall.
Bicuspid Aortic Valve
Do I need to be concerned with developing an aortic dissection?
Yes, the risk of aortic dissection is higher. In general, the risk is approximately 3 to 5 times higher than the general population. However, a contemporary study from Mount Sinai and Mayo groups indicated that the risk of aortic dissection was quite low in a population of bicuspid aortic valve patients followed carefully in an aortic surveillance program.
When should the ascending aortic aneurysm be considered for elective repair?
The criterion for elective surgery is based on expert opinion rather than concrete medical evidence. Regardless, most patients can be treated medically for a long period of time until either the valve or the size of the aorta dictate the need for surgery. Patients with moderate aortic dilatation can be followed with annual CT scans/MRI until the aorta increases to above 5 cm. However, various factors may need to be considered when treating a young patient such as the option of valve sparing aortic root replacement (David or Yacoub procedure), valve repair, rate of growth of the aorta, choice of valve prosthesis, and lifestyle. An important factor to consider is family history of aortic aneurysms and aortic dissections. A strong family history of aortic dissections or sudden death should lead to an earlier discussion regarding surgery.
When should the aorta be addressed if you are having an aortic valve replacement or another type of cardiac surgery?
If you are having surgery for dysfunction of the aortic valve, the ascending aorta should be replaced if the diameter is between 4.0 and 4.5 cm. There is some evidence to suggest that patients whom the surgeon did not replace the aorta at the initial surgery had a higher rate of aortic complications and need for additional cardiac surgery.
Should I participate in an aortic aneurysm surveillance program?
Yes, patients with a bicuspid aortic valve need careful follow-up by their cardiologist for annual echocardiograms and measurements of the ascending aorta either by CT scan or MRI. Once the ascending aortic diameter is equal to or greater than 4.0 cm the patient should have annual imaging studies. Aortic centers have surveillance programs available to carefully follow aortic aneurysms.
To sign up for our Aortic Surveillance Program.
Yes, the risk of aortic dissection is higher. In general, the risk is approximately 3 to 5 times higher than the general population. However, a contemporary study from Mount Sinai and Mayo groups indicated that the risk of aortic dissection was quite low in a population of bicuspid aortic valve patients followed carefully in an aortic surveillance program.
When should the ascending aortic aneurysm be considered for elective repair?
The criterion for elective surgery is based on expert opinion rather than concrete medical evidence. Regardless, most patients can be treated medically for a long period of time until either the valve or the size of the aorta dictate the need for surgery. Patients with moderate aortic dilatation can be followed with annual CT scans/MRI until the aorta increases to above 5 cm. However, various factors may need to be considered when treating a young patient such as the option of valve sparing aortic root replacement (David or Yacoub procedure), valve repair, rate of growth of the aorta, choice of valve prosthesis, and lifestyle. An important factor to consider is family history of aortic aneurysms and aortic dissections. A strong family history of aortic dissections or sudden death should lead to an earlier discussion regarding surgery.
When should the aorta be addressed if you are having an aortic valve replacement or another type of cardiac surgery?
If you are having surgery for dysfunction of the aortic valve, the ascending aorta should be replaced if the diameter is between 4.0 and 4.5 cm. There is some evidence to suggest that patients whom the surgeon did not replace the aorta at the initial surgery had a higher rate of aortic complications and need for additional cardiac surgery.
Should I participate in an aortic aneurysm surveillance program?
Yes, patients with a bicuspid aortic valve need careful follow-up by their cardiologist for annual echocardiograms and measurements of the ascending aorta either by CT scan or MRI. Once the ascending aortic diameter is equal to or greater than 4.0 cm the patient should have annual imaging studies. Aortic centers have surveillance programs available to carefully follow aortic aneurysms.
To sign up for our Aortic Surveillance Program.
