DESCENDING THORACIC AORTIC
ANEURYSMS
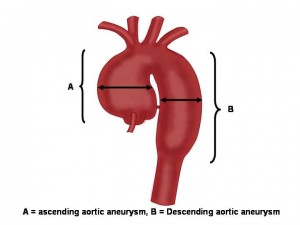
Descending thoracic aortic aneurysms are the third most common aortic aneurysm. The majority of patients are diagnosed in their 6th and 7th decade of life. Most patients are asymptomatic for a long period of time until the thoracic aortic disease is very advanced or found incidentally on a chest CT or MRI. The descending thoracic aorta is located in the posterior thorax (back of your chest caviy). As the aortic arch curves from the front portion of the thorax towards the back the descending thoracic aorta continues down the posterior portion of the chest cavity (refer to anatomy of the aorta). Please refer to the anatomy section for the illustration of the aorta. The anatomical boundaries of the descending thoracic aorta are the left subclavian artery and the celiac artery (this is the first major artery in the abdominal cavity). The location of the descending aorta provides some insight into the symptoms one may experience if there is a problem in this portion of the aorta.
Common causes of aortic aneurysms of the descending aorta included atherosclerosis, dissection, atherosclerotic plaque, infection, and connective tissue disorders. Theses aortic diseases are discussed in further detail in their respective section.
The presentation for the majority of descending aortic diseases is back pain or vague chest pain. Other symptoms include difficulty swallowing, hoarseness, and difficulty breathing (compression on the left main airway) and cough.
The plain chest x-ray can be a great first line diagnostic tool to indentify problems with the descending thoracic aorta. The chest x-ray may show that the heart shadow is widened and an exaggeration of the aortic contour. The gold standard to diagnosis descending thoracic aortic problems has become the CT scan with angiogram and MR angiogram. A transesophageal echocardiogram can detail the approximate size of the aorta and the presence of a dissection.
A majority of descending thoracic aortic diseases can be treated conservatively. When we speak of conservative management this refers to blood pressure control, aerobic exercise, smoking cessation, cholesterol control, and avoiding heavy weight lifting. However, symptoms related to a descending aortic aneurysm or dissection should be taken seriously.
The gold standard for repair of descending aortic aneurysms is open surgical repair. However, certain diseases of the descending thoracic aorta lend themselves to endovascular therapies. In addition, patients who are old and frail and with many medical problems, specifically, severe heart and lung problems may do better with endovascular stenting of the descending aorta. However, many factors are considered prior to making any recommendations for either approach.
The presentation for the majority of descending aortic diseases is back pain or vague chest pain. Other symptoms include difficulty swallowing, hoarseness, and difficulty breathing (compression on the left main airway) and cough.
The plain chest x-ray can be a great first line diagnostic tool to indentify problems with the descending thoracic aorta. The chest x-ray may show that the heart shadow is widened and an exaggeration of the aortic contour. The gold standard to diagnosis descending thoracic aortic problems has become the CT scan with angiogram and MR angiogram. A transesophageal echocardiogram can detail the approximate size of the aorta and the presence of a dissection.
A majority of descending thoracic aortic diseases can be treated conservatively. When we speak of conservative management this refers to blood pressure control, aerobic exercise, smoking cessation, cholesterol control, and avoiding heavy weight lifting. However, symptoms related to a descending aortic aneurysm or dissection should be taken seriously.
The gold standard for repair of descending aortic aneurysms is open surgical repair. However, certain diseases of the descending thoracic aorta lend themselves to endovascular therapies. In addition, patients who are old and frail and with many medical problems, specifically, severe heart and lung problems may do better with endovascular stenting of the descending aorta. However, many factors are considered prior to making any recommendations for either approach.
