Marfan Syndrome and the Aorta
**New public announcement from the Marfan Foundation.**
Marfan syndrome affects both genders and has been found among people of all races and ethnic backgrounds. It is estimated that at least 1 in 5,000 individuals in the United States are affected. Marfan Syndrome is caused by a gene mutation that results in abnormal connective tissue.
Connective tissue is found all over the body and is the skeleton/framework of most organ systems. Connective tissue makes up a variety of physical structures including tendons and the connective framework of fibers in muscles, ligaments, cartilage, skin and vascular system. Hence, many organ systems can be affected in an individual with Marfan syndrome such as the eyes, skeleton, skin, covering of the spinal cord, heart valves, blood vessels and teeth.
The diagnosis of Marfan Syndrome is based on a number of physical characteristics, supported by imaging studies and molecular testing. The revisted (2010) Ghent nosology is based on a point system evaluating major and minor manifestations (signs and symtoms) of Marfan syndome. A greater emphasis has been placed on the presence of an aortic root aneurysm, ectopia lentis and genetic testing. If you visit the Marfan Foundation website you can use their on-line calculator which uses a variety of features of Marfan syndrome to give you a probability score that you may have the disease.
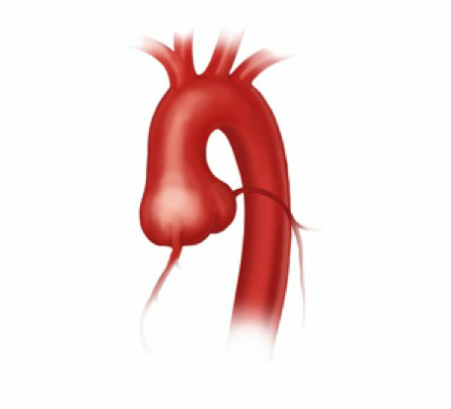
The primary purpose of connective tissue is to function as the framework of all organ systems and is instrumental in cell growth and development. The defective connective tissue in Marfan syndrome can affect many organ systems however, its effects on blood vessels – in particular on the aorta – can be life threatening. Since connective tissue provides the tensile strength of the aortic wall, the lack of structural support to the aorta can lead to the formation of an aneurysm and aortic dissection. The risk of rupture increases with the diameter of the aorta and therefore all patients with Marfan syndrome or other connective tissue disorders should be followed closely for expansion of the aorta. The most common place for aneurysms to occur in Marfan patients is at the level of the aortic root. As the aortic root aneurysm expands, this can cause insufficiency (leakage) of the aortic valve and eventually lead to symptoms like shortness of breath, fatigue, and chest pain. The second most common area for a Marfan patient to develop an aneurysm is at the level of the abdomen aorta. Once the aorta of a Marfan patient is dissected urgent surgical intervention is necessary. The diameter of aorta in which rupture or dissection may occur is much smaller than patients without a connective tissue disorder.
Once the aortic root diameter reaches 5 cm, the patient should be offered elective repair to prevent an acute aortic dissection. The best option for Marfan patient is a valve-sparing aortic root replacement or otherwise known as a David procedure. Superior, long-term results can be attained when there is minimal, pre-operative aortic valve regurgitation. Once the pre-operative aortic valve regurgitation increases then the long-term durability of the operation is less optimal.
To sign up for our Aortic Surveillance Program.
Marfan syndrome affects both genders and has been found among people of all races and ethnic backgrounds. It is estimated that at least 1 in 5,000 individuals in the United States are affected. Marfan Syndrome is caused by a gene mutation that results in abnormal connective tissue.
Connective tissue is found all over the body and is the skeleton/framework of most organ systems. Connective tissue makes up a variety of physical structures including tendons and the connective framework of fibers in muscles, ligaments, cartilage, skin and vascular system. Hence, many organ systems can be affected in an individual with Marfan syndrome such as the eyes, skeleton, skin, covering of the spinal cord, heart valves, blood vessels and teeth.
The diagnosis of Marfan Syndrome is based on a number of physical characteristics, supported by imaging studies and molecular testing. The revisted (2010) Ghent nosology is based on a point system evaluating major and minor manifestations (signs and symtoms) of Marfan syndome. A greater emphasis has been placed on the presence of an aortic root aneurysm, ectopia lentis and genetic testing. If you visit the Marfan Foundation website you can use their on-line calculator which uses a variety of features of Marfan syndrome to give you a probability score that you may have the disease.
The primary purpose of connective tissue is to function as the framework of all organ systems and is instrumental in cell growth and development. The defective connective tissue in Marfan syndrome can affect many organ systems however, its effects on blood vessels – in particular on the aorta – can be life threatening. Since connective tissue provides the tensile strength of the aortic wall, the lack of structural support to the aorta can lead to the formation of an aneurysm and aortic dissection. The risk of rupture increases with the diameter of the aorta and therefore all patients with Marfan syndrome or other connective tissue disorders should be followed closely for expansion of the aorta. The most common place for aneurysms to occur in Marfan patients is at the level of the aortic root. As the aortic root aneurysm expands, this can cause insufficiency (leakage) of the aortic valve and eventually lead to symptoms like shortness of breath, fatigue, and chest pain. The second most common area for a Marfan patient to develop an aneurysm is at the level of the abdomen aorta. Once the aorta of a Marfan patient is dissected urgent surgical intervention is necessary. The diameter of aorta in which rupture or dissection may occur is much smaller than patients without a connective tissue disorder.
Once the aortic root diameter reaches 5 cm, the patient should be offered elective repair to prevent an acute aortic dissection. The best option for Marfan patient is a valve-sparing aortic root replacement or otherwise known as a David procedure. Superior, long-term results can be attained when there is minimal, pre-operative aortic valve regurgitation. Once the pre-operative aortic valve regurgitation increases then the long-term durability of the operation is less optimal.
To sign up for our Aortic Surveillance Program.
