Highlights:
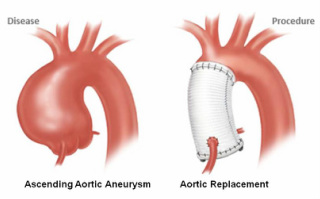
Ascending aortic aneurysms
1. In general, slow growing aneurysms
2. Healthy style and blood pressure control highly recommended
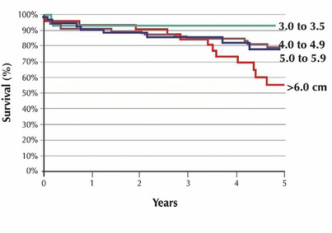
3. Surgery needed at diameter 5.5 cm or if growth > 1/2 cm in one year
4. Patients with connective tissue disorder or family history surgery at smaller diameter
5. Always consider second opinion at an Aortic Center before proceeding with surgery
1. In general, slow growing aneurysms
2. Healthy style and blood pressure control highly recommended
3. Surgery needed at diameter 5.5 cm or if growth > 1/2 cm in one year
4. Patients with connective tissue disorder or family history surgery at smaller diameter
5. Always consider second opinion at an Aortic Center before proceeding with surgery